Page 311 of 1529
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 12:38 am
by Clogs
CM11 wrote:Clogs wrote:message #2527204 wrote:goeagles wrote:Tehui wrote:
Somebody tell Rudi what the near future could look like, if the place is not locked down.
US Infection & Death Rate
10 days ago - 4,373 - 75
9 days ago - 5,662 - 96
8 days ago - 8.074 - 122
7 days ago - 12,018 - 174
6 days ago - 17,439 - 229
5 days ago - 23,710 - 296
4 days ago - 32,341 - 405
3 days ago - 42,749 - 516
2 days ago - 52,685 - 670
1 day ago - 64,661 - 929
today - 79,313 - 1,081
We've been doubling every 3 days in the total number of deaths. It's very unlikely to happen, but if we doubled every 3 days for a month (starting with the current 1177 dead), we'd have 1.2 million dead a month from now.
And a further 11m requiring critical care.
And if you doubled for just one month more then all of America would be dead and a further 3 billion requiring critical care.
So you've figured out that it'll run out of speed within two months leaving millions of Americans dead and 10s of millions in critical care. Well done.

Oh wait, there aren't 10s of millions of critical beds so change that millions dead to 10s of millions.

Way to miss the obvious sarcastic point.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 12:40 am
by Enzedder
CM11 wrote:Clogs wrote:
So you've figured out that it'll run out of speed within two months leaving millions of Americans dead and 10s of millions in critical care. Well done.
Oh wait, there aren't 10s of millions of critical beds so change that millions dead to 10s of millions.
Clogsy doesn't care as long as the BottleO is still open and he can get a haircut.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 12:42 am
by JM2K6
hermes-trismegistus wrote:eldanielfire wrote:Interesting tid bit. My friend works as a doctor in a Kent hospital. She says that they still have no masks/PPE. SO the command is do not resuscitate, because doing so could leave the recovered patient coffin out viral particles over non-protected staff. I wondering why haven't the hospitals got their PPE yet? The government claim they have been distributing it all week.
Also the the doctors who are working on the Coronavirus the longest have become seriously ill with it. The new thinking is while the old are most vulnerable for the young it's the volume of viral particles you absorb that matters. Which might be bad for NHS staff.
Viral load. I was reading a paper on this earlier. Seems to be the case that the heavier the exposure the heavier the illness in respect of things like SARS, CV, etc. Makes sense I suppose. Although I have to admit, I’d previously thought from what I’d been hearing that a fleeting brush against an infected door handle was every bit as dangerous as a pair of infectees coughing in your face for ten minutes. Apparently not so clearcut. Grey areas.
Door handle -> touching face = you get infected.
How badly you handle being infected is down to a number of factors, not all of which are understood it seems, but increasing the viral load simply makes it harder for your body to fight it.
Which is why if you're sharing a place with someone, if they get sick you shouldn't just go "oh well I guess I'll be getting it" - you have to try and isolate them because if you do get sick, the two of you do not want to be increasing the viral load for each other.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 12:42 am
by JM2K6
Clogs wrote:Way to miss the obvious sarcastic point.
What is it about exponential growth that you're not getting?
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 12:46 am
by Clogs
JM2K6 wrote:Clogs wrote:Again, Wuhan's figures were death rate/confirmed cases = 3.4%. This is a grossly flawed equation. Confirmed cases (those that were tested) was an order of magnitude lower than those that were/are actually infected. To get the true death rate you need to have the true infected rate. Something that is impossible to do, but epidemiologists are nowstarting to model. And gradually they are starting to agree that this % death rate could be far far far below what is currently reported.
Reporting the case fatality rate (as opposed to the death rate in total) is de rigeur here, it's not the gotcha you think it is. A CFR of >1% with a virus that has an R0 of somewhere between 2.5 and 3 is a lot of dead people. No-one really cares about the "true death rate", it's kinda irrelevant to anyone trying to treat it.
Good point, but what it does help with is actually planning for your worst case scenario a lot more accurately. There is a natural high water mark with infections. If you can calculate the infection rate, then apply the recovery rate(herd immunity) then apply the % gravely ill (at risk of death) it allows you to predict when the worst will occur and what it will look like and allow you to plan accordingly.
If the actual death rate is 1% then we are fvcked. However none of the data is starting to back that up. If anything the modelling is starting to show that it is magnitutdes lower than that. When applied to Italy you can see they have already peaked (as most of their population was likely infected before lockdown) and with social distancing and herd immunity they are almost out of the woods. Estimates are showing that Italy has millions that have been infected (and many/most will have recovered - if the virus is out of our system in 14 days). They will not suffer millions of deaths.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 12:58 am
by Clogs
JM2K6 wrote:Clogs wrote:Way to miss the obvious sarcastic point.
What is it about exponential growth that you're not getting?
Well there is exponential growth up to a limit. In the ridiculous example I provided, I was trying to show that simply applying exponential growth to this problem is not how it works. If it did then all of America would be dead and 3 Billion more Americans would need intensive care...
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 1:01 am
by Clogs
JM2K6 wrote:Clogs wrote:Way to miss the obvious sarcastic point.
What is it about exponential growth that you're not getting?
I have tried to model the exponential growth. I have also tried to add in the recovery rate. Because as that increases that should dramatically slow the number of infections (herd immunity). If you apply this logic to Italy and then work out their death rate you may get an idea of just how many people are or have been infected. This is back of the envelope stuff.

Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 1:04 am
by TheFrog
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 1:06 am
by Clogs
Enzedder wrote:CM11 wrote:Clogs wrote:
So you've figured out that it'll run out of speed within two months leaving millions of Americans dead and 10s of millions in critical care. Well done.
Oh wait, there aren't 10s of millions of critical beds so change that millions dead to 10s of millions.
Clogsy doesn't care as long as the BottleO is still open and he can get a haircut.
Fvck that. I can wear a ponytail if I have to. If you cose the Bottle-O we will have fvcking riots! I will lead the charge.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 1:30 am
by goeagles
Clogs wrote:JM2K6 wrote:Clogs wrote:Way to miss the obvious sarcastic point.
What is it about exponential growth that you're not getting?
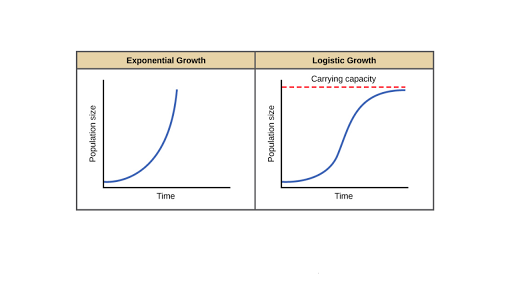
Well there is exponential growth up to a limit. In the ridiculous example I provided, I was trying to show that simply applying exponential growth to this problem is not how it works. If it did then all of America would be dead and 3 Billion more Americans would need intensive care...
Viruses follow logistic growth curves. Logistic curves are very close to exponential growth in early stages, which we still are in as a very low percentage of people have actually caught the virus.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 1:30 am
by Yer Man
comets wrote:USA officially passes China as the most infected..... now Xing Ji will call it the American virus
I thought Trümp wanted to stop imports from China
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 1:36 am
by Clogs
goeagles wrote:Clogs wrote:JM2K6 wrote:Clogs wrote:Way to miss the obvious sarcastic point.
What is it about exponential growth that you're not getting?
Well there is exponential growth up to a limit. In the ridiculous example I provided, I was trying to show that simply applying exponential growth to this problem is not how it works. If it did then all of America would be dead and 3 Billion more Americans would need intensive care...
Viruses follow logistic growth curves. Logistic curves are very close to exponential growth in early stages, which
we still are in as a very low percentage of people have actually caught the virus.
Are you sure?
The epidemic started in China sometime in November or December. The first confirmed U.S. cases included a person who traveled from Wuhan on Jan. 15, and it is likely that the virus entered before that: Tens of thousands of people traveled from Wuhan to the U.S. in December. Existing evidence suggests that the virus is highly transmissible and that the number of infections doubles roughly every three days. An epidemic seed on Jan. 1 implies that by March 9 about six million people in the U.S. would have been infected. As of March 23, according to the Centers for Disease Control and Prevention, there were 499 Covid-19 deaths in the U.S. If our surmise of six million cases is accurate, that’s a mortality rate of 0.01%, assuming a two week lag between infectio
Dr. Bendavid and Dr. Bhattacharya are professors of medicine at Stanford. Neeraj Sood contributed to this article
Some very smart people seem to think the infection rate is actually quite high...
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 1:53 am
by TheFrog
The question is therefore: if a large amount of the population is or has been infected and the virus is therefore not the lethal, why are hospitals saturated with severe cases and why do we see daily more deaths than during a flu epidemic?
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 1:53 am
by Sensible Stephen
Clogs wrote:goeagles wrote:Clogs wrote:JM2K6 wrote:Clogs wrote:Way to miss the obvious sarcastic point.
What is it about exponential growth that you're not getting?
Well there is exponential growth up to a limit. In the ridiculous example I provided, I was trying to show that simply applying exponential growth to this problem is not how it works. If it did then all of America would be dead and 3 Billion more Americans would need intensive care...
Viruses follow logistic growth curves. Logistic curves are very close to exponential growth in early stages, which
we still are in as a very low percentage of people have actually caught the virus.
Are you sure?
The epidemic started in China sometime in November or December. The first confirmed U.S. cases included a person who traveled from Wuhan on Jan. 15, and it is likely that the virus entered before that: Tens of thousands of people traveled from Wuhan to the U.S. in December. Existing evidence suggests that the virus is highly transmissible and that the number of infections doubles roughly every three days. An epidemic seed on Jan. 1 implies that by March 9 about six million people in the U.S. would have been infected. As of March 23, according to the Centers for Disease Control and Prevention, there were 499 Covid-19 deaths in the U.S. If our surmise of six million cases is accurate, that’s a mortality rate of 0.01%, assuming a two week lag between infectio
Dr. Bendavid and Dr. Bhattacharya are professors of medicine at Stanford. Neeraj Sood contributed to this article
Some very smart people seem to think the infection rate is actually quite high...
I am sure well all hope that is the case, as that would be great.
But look at the Korean data. Look at the death rates there. The Korean data is probably the most accurate data we have right now due to the range and scope of their testing. Their death rate is 1.4%. 13.6% in those over 80, 6.4% in those over 70, 1.7% in those over 60. Those are not numbers to just wave away.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 1:58 am
by Clogs
TheFrog wrote:The question is therefore: if a large amount of the population is or has been infected and the virus is therefore not the lethal, why are hospitals saturated with severe cases and why do we see daily more deaths than during a flu epidemic?
Volume of infections x % that do end up critical = saturation. But it is a shorter saturation not one that plays out over months.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 1:58 am
by goeagles
Clogs wrote:goeagles wrote:Clogs wrote:JM2K6 wrote:Clogs wrote:Way to miss the obvious sarcastic point.
What is it about exponential growth that you're not getting?
Well there is exponential growth up to a limit. In the ridiculous example I provided, I was trying to show that simply applying exponential growth to this problem is not how it works. If it did then all of America would be dead and 3 Billion more Americans would need intensive care...
Viruses follow logistic growth curves. Logistic curves are very close to exponential growth in early stages, which
we still are in as a very low percentage of people have actually caught the virus.
Are you sure?
The epidemic started in China sometime in November or December. The first confirmed U.S. cases included a person who traveled from Wuhan on Jan. 15, and it is likely that the virus entered before that: Tens of thousands of people traveled from Wuhan to the U.S. in December. Existing evidence suggests that the virus is highly transmissible and that the number of infections doubles roughly every three days. An epidemic seed on Jan. 1 implies that by March 9 about six million people in the U.S. would have been infected. As of March 23, according to the Centers for Disease Control and Prevention, there were 499 Covid-19 deaths in the U.S. If our surmise of six million cases is accurate, that’s a mortality rate of 0.01%, assuming a two week lag between infectio
Dr. Bendavid and Dr. Bhattacharya are professors of medicine at Stanford. Neeraj Sood contributed to this article
Some very smart people seem to think the infection rate is actually quite high...
What are their qualifications? Can you link the whole article? There is one major mistake I can see from that alone which is failure to account for virus spread distribution being fat-tailed. Two week lag from infection to death also seems a dubious assumption but I haven't seen any data on that.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 1:59 am
by Blackrock Bullet
TheFrog wrote:The question is therefore: if a large amount of the population is or has been infected and the virus is therefore not the lethal, why are hospitals saturated with severe cases and why do we see daily more deaths than during a flu epidemic?
Because we’re at the peak and the R level is so high?
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 2:00 am
by TheFrog
Clogs wrote:TheFrog wrote:The question is therefore: if a large amount of the population is or has been infected and the virus is therefore not the lethal, why are hospitals saturated with severe cases and why do we see daily more deaths than during a flu epidemic?
Volume of infections x % that do end up critical = saturation. But it is a shorter saturation not one that plays out over months.
Still means a lot of people who could have been saved will die.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 2:02 am
by TheFrog
Blackrock Bullet wrote:TheFrog wrote:The question is therefore: if a large amount of the population is or has been infected and the virus is therefore not the lethal, why are hospitals saturated with severe cases and why do we see daily more deaths than during a flu epidemic?
Because we’re at the peak and the R level is so high?
Then we'll get a proof of this as soon as they let people out again. If we see the same hyperbolic curve of contaminations and deaths, then we were not yet at the peak and we have a longer term problem.
But in any case, short term confinement makes sense to ease the pressure on hospitals.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 2:04 am
by goeagles
Sensible Stephen wrote:Clogs wrote:goeagles wrote:Clogs wrote:JM2K6 wrote:
What is it about exponential growth that you're not getting?
Well there is exponential growth up to a limit. In the ridiculous example I provided, I was trying to show that simply applying exponential growth to this problem is not how it works. If it did then all of America would be dead and 3 Billion more Americans would need intensive care...
Viruses follow logistic growth curves. Logistic curves are very close to exponential growth in early stages, which
we still are in as a very low percentage of people have actually caught the virus.
Are you sure?
The epidemic started in China sometime in November or December. The first confirmed U.S. cases included a person who traveled from Wuhan on Jan. 15, and it is likely that the virus entered before that: Tens of thousands of people traveled from Wuhan to the U.S. in December. Existing evidence suggests that the virus is highly transmissible and that the number of infections doubles roughly every three days. An epidemic seed on Jan. 1 implies that by March 9 about six million people in the U.S. would have been infected. As of March 23, according to the Centers for Disease Control and Prevention, there were 499 Covid-19 deaths in the U.S. If our surmise of six million cases is accurate, that’s a mortality rate of 0.01%, assuming a two week lag between infectio
Dr. Bendavid and Dr. Bhattacharya are professors of medicine at Stanford. Neeraj Sood contributed to this article
Some very smart people seem to think the infection rate is actually quite high...
I am sure well all hope that is the case, as that would be great.
But look at the Korean data. Look at the death rates there. The Korean data is probably the most accurate data we have right now due to the range and scope of their testing. Their death rate is 1.4%. 13.6% in those over 80, 6.4% in those over 70, 1.7% in those over 60. Those are not numbers to just wave away.
Antibody tests are going to be very interesting. We don't know how many people are asymptomatic carriers who never show symptoms. Even with Korea's widespread testing, it's more for people who think they either have it or have been exposed to someone who has it. There may be many more who are asymptomatic carriers who never knew they had it in the first place. Still, that's not something we can bank on for policy.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 2:19 am
by Clogs
goeagles wrote:
What are their qualifications? Can you link the whole article? There is one major mistake I can see from that alone which is failure to account for virus spread distribution being fat-tailed. Two week lag from infection to death also seems a dubious assumption but I haven't seen any data on that.
https://www.wsj.com/articles/is-the-cor ... 1585088464
Is the Coroavirus as deadly as they Say?
Current estimates about the Covid-19 fatality rate may be too high by orders of magnitude.
By
Eran Bendavid and
Jay Bhattacharya
March 24, 2020 6:21 pm ET
A line at an emergency room in Brooklyn, N.Y., March 19.PHOTO: ANDREW KELLY/REUTERS
If it’s true that the novel coronavirus would kill millions without shelter-in-place orders and quarantines, then the extraordinary measures being carried out in cities and states around the country are surely justified. But there’s little evidence to confirm that premise—and projections of the death toll could plausibly be orders of magnitude too high.
Fear of Covid-19 is based on its high estimated case fatality rate—2% to 4% of people with confirmed Covid-19 have died, according to the World Health Organization and others. So if 100 million Americans ultimately get the disease, two million to four million could die. We believe that estimate is deeply flawed. The true fatality rate is the portion of those infected who die, not the deaths from identified positive cases.
The latter rate is misleading because of selection bias in testing. The degree of bias is uncertain because available data are limited. But it could make the difference between an epidemic that kills 20,000 and one that kills two million. If the number of actual infections is much larger than the number of cases—orders of magnitude larger—then the true fatality rate is much lower as well. That’s not only plausible but likely based on what we know so far.
Population samples from China, Italy, Iceland and the U.S. provide relevant evidence. On or around Jan. 31, countries sent planes to evacuate citizens from Wuhan, China. When those planes landed, the passengers were tested for Covid-19 and quarantined. After 14 days, the percentage who tested positive was 0.9%. If this was the prevalence in the greater Wuhan area on Jan. 31, then, with a population of about 20 million, greater Wuhan had 178,000 infections, about 30-fold more than the number of reported cases. The fatality rate, then, would be at least 10-fold lower than estimates based on reported cases.
Next, the northeastern Italian town of Vò, near the provincial capital of Padua. On March 6, all 3,300 people of Vò were tested, and 90 were positive, a prevalence of 2.7%. Applying that prevalence to the whole province (population 955,000), which had 198 reported cases, suggests there were actually 26,000 infections at that time. That’s more than 130-fold the number of actual reported cases. Since Italy’s case fatality rate of 8% is estimated using the confirmed cases, the real fatality rate could in fact be closer to 0.06%.
ADVERTISEMENT
In Iceland, deCode Genetics is working with the government to perform widespread testing. In a sample of nearly 2,000 entirely asymptomatic people, researchers estimated disease prevalence of just over 1%. Iceland’s first case was reported on Feb. 28, weeks behind the U.S. It’s plausible that the proportion of the U.S. population that has been infected is double, triple or even 10 times as high as the estimates from Iceland. That also implies a dramatically lower fatality rate.
The best (albeit very weak) evidence in the U.S. comes from the National Basketball Association. Between March 11 and 19, a substantial number of NBA players and teams received testing. By March 19, 10 out of 450 rostered players were positive. Since not everyone was tested, that represents a lower bound on the prevalence of 2.2%. The NBA isn’t a representative population, and contact among players might have facilitated transmission. But if we extend that lower-bound assumption to cities with NBA teams (population 45 million), we get at least 990,000 infections in the U.S. The number of cases reported on March 19 in the U.S. was 13,677, more than 72-fold lower. These numbers imply a fatality rate from Covid-19 orders of magnitude smaller than it appears.
How can we reconcile these estimates with the epidemiological models? First, the test used to identify cases doesn’t catch people who were infected and recovered. Second, testing rates were woefully low for a long time and typically reserved for the severely ill. Together, these facts imply that the confirmed cases are likely orders of magnitude less than the true number of infections. Epidemiological modelers haven’t adequately adapted their estimates to account for these factors.
The epidemic started in China sometime in November or December. The first confirmed U.S. cases included a person who traveled from Wuhan on Jan. 15, and it is likely that the virus entered before that: Tens of thousands of people traveled from Wuhan to the U.S. in December. Existing evidence suggests that the virus is highly transmissible and that the number of infections doubles roughly every three days. An epidemic seed on Jan. 1 implies that by March 9 about six million people in the U.S. would have been infected. As of March 23, according to the Centers for Disease Control and Prevention, there were 499 Covid-19 deaths in the U.S. If our surmise of six million cases is accurate, that’s a mortality rate of 0.01%, assuming a two week lag between infection and death. This is one-tenth of the flu mortality rate of 0.1%. Such a low death rate would be cause for optimism.
ADVERTISEMENT
This does not make Covid-19 a nonissue. The daily reports from Italy and across the U.S. show real struggles and overwhelmed health systems. But a 20,000- or 40,000-death epidemic is a far less severe problem than one that kills two million. Given the enormous consequences of decisions around Covid-19 response, getting clear data to guide decisions now is critical. We don’t know the true infection rate in the U.S. Antibody testing of representative samples to measure disease prevalence (including the recovered) is crucial. Nearly every day a new lab gets approval for antibody testing, so population testing using this technology is now feasible.
If we’re right about the limited scale of the epidemic, then measures focused on older populations and hospitals are sensible. Elective procedures will need to be rescheduled. Hospital resources will need to be reallocated to care for critically ill patients. Triage will need to improve. And policy makers will need to focus on reducing risks for older adults and people with underlying medical conditions.
A universal quarantine may not be worth the costs it imposes on the economy, community and individual mental and physical health. We should undertake immediate steps to evaluate the empirical basis of the current lockdowns.
Dr. Bendavid and Dr. Bhattacharya are professors of medicine at Stanford. Neeraj Sood contributed to this article.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 2:25 am
by Clogs
Sensible Stephen wrote:
I am sure well all hope that is the case, as that would be great.
But look at the Korean data. Look at the death rates there. The Korean data is probably the most accurate data we have right now due to the range and scope of their testing. Their death rate is 1.4%. 13.6% in those over 80, 6.4% in those over 70, 1.7% in those over 60. Those are not numbers to just wave away.
Australia's scope of testing has been pretty sound...
Over 180 000 tests (might be the most per capita)
3 000 confirmed
13 deaths
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 2:28 am
by Clogs
goeagles wrote:
Antibody tests are going to be very interesting. We don't know how many people are asymptomatic carriers who never show symptoms. Even with Korea's widespread testing, it's more for people who think they either have it or have been exposed to someone who has it. There may be many more who are asymptomatic carriers who never knew they had it in the first place. Still, that's not something we can bank on for policy.
Yep. I think that is what the Oxford study is trying to find out. They have apparently got funding to get testing underway too. Fingers crossed it is very contagious (doubles every 3 days), 99.99% of infections are in fact mild and we can all practice sensible social distancing and hand washing in order to reduce the spread. Herd immunity would build up over a month or two and we are out of the woods.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 2:41 am
by Sensible Stephen
Clogs wrote:Sensible Stephen wrote:
I am sure well all hope that is the case, as that would be great.
But look at the Korean data. Look at the death rates there. The Korean data is probably the most accurate data we have right now due to the range and scope of their testing. Their death rate is 1.4%. 13.6% in those over 80, 6.4% in those over 70, 1.7% in those over 60. Those are not numbers to just wave away.
Australia's scope of testing has been pretty sound...
Over 180 000 tests (might be the most per capita)
3 000 confirmed
13 deaths
Its not the most per capita. Koreas number is 6k/million, UAE 12.7k/million, Australia 4k/million. Korea did mass testing when the numbers were low and testing far and wide. Australia has only just ramped up testing with the number of cases already being quite large.
Australia is early days. The death rate really seems to rocket once the hospitals become overwhelmed, lets hope that doesn't happen.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 2:56 am
by Clogs
Sensible Stephen wrote:Clogs wrote:Sensible Stephen wrote:
I am sure well all hope that is the case, as that would be great.
But look at the Korean data. Look at the death rates there. The Korean data is probably the most accurate data we have right now due to the range and scope of their testing. Their death rate is 1.4%. 13.6% in those over 80, 6.4% in those over 70, 1.7% in those over 60. Those are not numbers to just wave away.
Australia's scope of testing has been pretty sound...
Over 180 000 tests (might be the most per capita)
3 000 confirmed
13 deaths
Its not the most per capita. Koreas number is 6k/million, UAE 12.7k/million, Australia 4k/million. Korea did mass testing when the numbers were low and testing far and wide. Australia has only just ramped up testing with the number of cases already being quite large.
Australia is early days. The death rate really seems to rocket once the hospitals become overwhelmed, lets hope that doesn't happen.
On this point we totally agree. Let's hope. It is interesting to note the number of cases per day seems to be dropping, so we may have gotten ahead of it..?
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 2:57 am
by Sensible Stephen
Clogs wrote:goeagles wrote:
Antibody tests are going to be very interesting. We don't know how many people are asymptomatic carriers who never show symptoms. Even with Korea's widespread testing, it's more for people who think they either have it or have been exposed to someone who has it. There may be many more who are asymptomatic carriers who never knew they had it in the first place. Still, that's not something we can bank on for policy.
Yep. I think that is what the Oxford study is trying to find out. They have apparently got funding to get testing underway too. Fingers crossed it is very contagious (doubles every 3 days), 99.99% of infections are in fact mild and we can all practice sensible social distancing and hand washing in order to reduce the spread. Herd immunity would build up over a month or two and we are out of the woods.
I hope that is the case, but an overly cautious approach is far more sensible until we can do the wide ranging testing. And hopefully have those anti viral drugs going to stop severe cases in their tracks.
So far, not too bad for Australia. Lets hope the death rate stays low.
https://www.news.com.au/lifestyle/healt ... f3630d1030
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 3:01 am
by Sensible Stephen
Clogs wrote:
On this point we totally agree. Let's hope. It is interesting to note the number of cases per day seems to be dropping, so we may have gotten ahead of it..?
That would be nice. I went out yesterday to get a flu jab. The Adelaide central markets were packed, zero social isolating going on. 95% of the people would have been 60+ as well.

I think the number of cases in SA is 250ish. Definitely not peaked here, and a lot of scope for community transmission through those dumbass boomers.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 3:14 am
by Clogs
Sensible Stephen wrote:Clogs wrote:
On this point we totally agree. Let's hope. It is interesting to note the number of cases per day seems to be dropping, so we may have gotten ahead of it..?
That would be nice. I went out yesterday to get a flu jab.
The Adelaide central markets were packed, zero social isolating going on. 95% of the people would have been 60+ as well.
I think the number of cases in SA is 250ish. Definitely not peaked here, and a lot of scope for community transmission through those dumbass boomers.
WTF? Are South Australians really as thick as Queenslanders?
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 3:57 am
by paddyor
eldanielfire wrote:Interesting tid bit. My friend works as a doctor in a Kent hospital. She says that they still have no masks/PPE. SO the command is do not resuscitate, because doing so could leave the recovered patient coffin out viral particles over non-protected staff. I wondering why haven't the hospitals got their PPE yet? The government claim they have been distributing it all week.
Also the the doctors who are working on the Coronavirus the longest have become seriously ill with it. The new thinking is while the old are most vulnerable for the young it's the volume of viral particles you absorb that matters. Which might be bad for NHS staff.
I think the viral load theory has been debunked as of a few days ago. I'm not digging it out though.
WRT masks and other PPE. Surgeons don't wear them to protect themselves from patients, it's the other way around. Mask offer some protection vice versa but they wear them in Japan when they've a sniffle to protect others.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 4:03 am
by OptimisticJock
eldanielfire wrote:Interesting tid bit. My friend works as a doctor in a Kent hospital. She says that they still have no masks/PPE. SO the command is do not resuscitate, because doing so could leave the recovered patient coffin out viral particles over non-protected staff. I wondering why haven't the hospitals got their PPE yet? The government claim they have been distributing it all week.
Also the the doctors who are working on the Coronavirus the longest have become seriously ill with it. The new thinking is while the old are most vulnerable for the young it's the volume of viral particles you absorb that matters. Which might be bad for NHS staff.
I mentioned this pages ago. It's not quite DNR but no ventilations are to be carried out unless everyone has the correct PPE.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 4:56 am
by paddyor
JM2K6 wrote:hermes-trismegistus wrote:eldanielfire wrote:Interesting tid bit. My friend works as a doctor in a Kent hospital. She says that they still have no masks/PPE. SO the command is do not resuscitate, because doing so could leave the recovered patient coffin out viral particles over non-protected staff. I wondering why haven't the hospitals got their PPE yet? The government claim they have been distributing it all week.
Also the the doctors who are working on the Coronavirus the longest have become seriously ill with it. The new thinking is while the old are most vulnerable for the young it's the volume of viral particles you absorb that matters. Which might be bad for NHS staff.
Viral load. I was reading a paper on this earlier. Seems to be the case that the heavier the exposure the heavier the illness in respect of things like SARS, CV, etc. Makes sense I suppose. Although I have to admit, I’d previously thought from what I’d been hearing that a fleeting brush against an infected door handle was every bit as dangerous as a pair of infectees coughing in your face for ten minutes. Apparently not so clearcut. Grey areas.
Door handle -> touching face = you get infected.
How badly you handle being infected is down to a number of factors, not all of which are understood it seems, but increasing the viral load simply makes it harder for your body to fight it.
Which is why if you're sharing a place with someone, if they get sick you shouldn't just go "oh well I guess I'll be getting it" - you have to try and isolate them because if you do get sick, the two of you do not want to be increasing the viral load for each other.
That's not defo true. There's a lot of face to touch without injesting the virus and you need to transfer the cirus from your hand to face. It's not a bateria that will multiply and spread. THe primary driver outside imtimate relationships is people coughing and sneezing in enclosed areas.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 5:28 am
by MrJonno
With regards to the numbers I think a lot of people are taking a rather simplistic approach. Recently a man in his 90s in the Czech Republic who had numerous underlying health issues, was clining on to life and expected to expire any minute, caught covid 19 and then 'moved on'. There was some debate as to whether he should be considered a covid fatality and the medical consensus was he shouldn't because he was dying this week regardless of whether he caught it or not, and also, the official cause of death was one of his other major issues, but tin foil hat wearers are crying conspiracy (much like some on here with the German figures based on news stories and no further understanding).
As this affects the old and sweeps through hospitals there are going to be some people specifically killed by C19 but there are presumably going to be a not insignificant number of people who catch it and then die of whatever they were in there for in the first place, possibly at little earlier than otherwise expected but sometimes, presumably not.
It must be reasonably straight forward to account of the number of deaths that would be expected to occur without covid, for example, there must be a rough figure for how many elderly people are expected to die from flu, if the current number is half that I think it is a little disingenous to discount that in terms of the effect C19 is having on society.
The problem is with everyone on lock down there is no other news so the media are focusing on this and for some reason feel vindicated if they sensationalise something and then finish with a piece of people clapping nurses
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 5:55 am
by goeagles
Clogs wrote:goeagles wrote:Clogs wrote:JM2K6 wrote:Clogs wrote:Way to miss the obvious sarcastic point.
What is it about exponential growth that you're not getting?
Well there is exponential growth up to a limit. In the ridiculous example I provided, I was trying to show that simply applying exponential growth to this problem is not how it works. If it did then all of America would be dead and 3 Billion more Americans would need intensive care...
Viruses follow logistic growth curves. Logistic curves are very close to exponential growth in early stages, which
we still are in as a very low percentage of people have actually caught the virus.
Are you sure?
The epidemic started in China sometime in November or December. The first confirmed U.S. cases included a person who traveled from Wuhan on Jan. 15, and it is likely that the virus entered before that: Tens of thousands of people traveled from Wuhan to the U.S. in December. Existing evidence suggests that the virus is highly transmissible and that the number of infections doubles roughly every three days. An epidemic seed on Jan. 1 implies that by March 9 about six million people in the U.S. would have been infected. As of March 23, according to the Centers for Disease Control and Prevention, there were 499 Covid-19 deaths in the U.S. If our surmise of six million cases is accurate, that’s a mortality rate of 0.01%, assuming a two week lag between infectio
Dr. Bendavid and Dr. Bhattacharya are professors of medicine at Stanford. Neeraj Sood contributed to this article
Some very smart people seem to think the infection rate is actually quite high...
Had a little more time to think this through. Ignore the fact that spread is not evenly distributed (superspreaders make the distribution fat tailed), that their seed 2 weeks prior to first confirmed case is pulled out of thin air (which has a huge impact on their calculations), that growth is logistic not exponential or that the two week lag between initial infection and death is not only pulled out of thin air but doesn't make much sense from what we've heard.
Let's use their same exact methodology for Italy as they've used for the US. The first confirmed case in Italy was on January 31. So let's go back 2 weeks and make the seed case on January 17th. If we double the number of cases every 3 days until March 2nd, we get 32,768 cases. And if we use their 2 week lag between infection and death, we would use the number of deaths on March 16th, which was 2158. If we use their same methodology, even with all of its spurious assumptions, we get a death rate of 6.59%!
You can play around with those numbers and changes in assumptions (date of first seed case, average length from initial infection to death) make huge differences. If you change the average time from death to infection from 14 days to 23 days, you get a death rate of 25.07% in Italy, all else held constant, which is obviously bullshit. So is the death rate 6.59% in Italy and 0.01% in the US using their methodology. It makes no sense.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 6:18 am
by goeagles
MrJonno wrote:With regards to the numbers I think a lot of people are taking a rather simplistic approach. Recently a man in his 90s in the Czech Republic who had numerous underlying health issues, was clining on to life and expected to expire any minute, caught covid 19 and then 'moved on'. There was some debate as to whether he should be considered a covid fatality and the medical consensus was he shouldn't because he was dying this week regardless of whether he caught it or not, and also, the official cause of death was one of his other major issues, but tin foil hat wearers are crying conspiracy (much like some on here with the German figures based on news stories and no further understanding).
As this affects the old and sweeps through hospitals there are going to be some people specifically killed by C19 but there are presumably going to be a not insignificant number of people who catch it and then die of whatever they were in there for in the first place, possibly at little earlier than otherwise expected but sometimes, presumably not.
It must be reasonably straight forward to account of the number of deaths that would be expected to occur without covid, for example, there must be a rough figure for how many elderly people are expected to die from flu, if the current number is half that I think it is a little disingenous to discount that in terms of the effect C19 is having on society.
The problem is with everyone on lock down there is no other news so the media are focusing on this and for some reason feel vindicated if they sensationalise something and then finish with a piece of people clapping nurses
The COVID-19 official count also does not include people who die from other diseases because hospitals are overloaded and can't get adequate care as a result. When a heart attack patient who would have lived under normal conditions has to wait 2 hours and dies, that doesn't count in the COVID-19 stats.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 6:37 am
by Anonymous 1
Found out yesterday a friend of mines whole family got infected. That's wife two adult kids and the ancient in laws. They were self isolating at the in laws property with huge stock of food thinking everyone was healthy. Then one by one they all got a bit sick. Luckily the ancient in laws with all sorts of underlying health conditions are well enough to look after the rest of them.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 7:00 am
by frillage
Anonymous. wrote:Found out yesterday a friend of mines whole family got infected. That's wife two adult kids and the ancient in laws. They were self isolating at the in laws property with huge stock of food thinking everyone was healthy. Then one by one they all got a bit sick. Luckily the ancient in laws with all sorts of underlying health conditions are well enough to look after the rest of them.
That’s one way to get rid of the mother in law, straight out of Globbies playbook.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 7:00 am
by Clogs
goeagles wrote:Clogs wrote:goeagles wrote:Clogs wrote:
Well there is exponential growth up to a limit. In the ridiculous example I provided, I was trying to show that simply applying exponential growth to this problem is not how it works. If it did then all of America would be dead and 3 Billion more Americans would need intensive care...
Viruses follow logistic growth curves. Logistic curves are very close to exponential growth in early stages, which
we still are in as a very low percentage of people have actually caught the virus.
Are you sure?
The epidemic started in China sometime in November or December. The first confirmed U.S. cases included a person who traveled from Wuhan on Jan. 15, and it is likely that the virus entered before that: Tens of thousands of people traveled from Wuhan to the U.S. in December. Existing evidence suggests that the virus is highly transmissible and that the number of infections doubles roughly every three days. An epidemic seed on Jan. 1 implies that by March 9 about six million people in the U.S. would have been infected. As of March 23, according to the Centers for Disease Control and Prevention, there were 499 Covid-19 deaths in the U.S. If our surmise of six million cases is accurate, that’s a mortality rate of 0.01%, assuming a two week lag between infectio
Dr. Bendavid and Dr. Bhattacharya are professors of medicine at Stanford. Neeraj Sood contributed to this article
Some very smart people seem to think the infection rate is actually quite high...
Had a little more time to think this through. Ignore the fact that spread is not evenly distributed (superspreaders make the distribution fat tailed), that their seed 2 weeks prior to first confirmed case is pulled out of thin air (which has a huge impact on their calculations), that growth is logistic not exponential or that the two week lag between initial infection and death is not only pulled out of thin air but doesn't make much sense from what we've heard.
Let's use their same exact methodology for Italy as they've used for the US. The first confirmed case in Italy was on January 31. So let's go back 2 weeks and make the seed case on January 17th. If we double the number of cases every 3 days until March 2nd, we get 32,768 cases. And if we use their 2 week lag between infection and death, we would use the number of deaths on March 16th, which was 2158. If we use their same methodology, even with all of its spurious assumptions, we get a death rate of 6.59%!
You can play around with those numbers and changes in assumptions (date of first seed case, average length from initial infection to death) make huge differences. If you change the average time from death to infection from 14 days to 23 days, you get a death rate of 25.07% in Italy, all else held constant, which is obviously bullshit. So is the death rate 6.59% in Italy and 0.01% in the US using their methodology. It makes no sense.
I think where you are getting to is that the first case in Italy was way way before the 31st of Jan. Even way before the 15th of Jan.
Some high tech Photoshop work to visually demonstrate...

Based on this superb photoshop, the blue is what people think is the infected rate (largely due to testing) but the red and blue is the actual because the seed case was way way earlier than detected. Italy's death rate much higher because their seed date was so much earlier. Same for Spain. South Korea got onto it early, as it appears has NZ and hopefully Australia.
Reverese engineer a 0.1% death rate and you get the infected rate. Reverse engineer a 1% death rate and you can get the infected rate. You constant (and accurately measured) is the death rate. At 0.1% reverse engineered it show Italy was massively infected. We will know if this was true if their total number of deaths start dropping (is it because of isolation or because they actually suffered such a high infection rate withouth knowing). I tend to think their population was massively infected hence the high total deaths relative to other countries. Sadly that may play out for the US before they turn the corner because even a 0.1% death rate on a hugely infected population is tens of thousands dead...
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 7:18 am
by MrJonno
goeagles wrote:MrJonno wrote:With regards to the numbers I think a lot of people are taking a rather simplistic approach. Recently a man in his 90s in the Czech Republic who had numerous underlying health issues, was clining on to life and expected to expire any minute, caught covid 19 and then 'moved on'. There was some debate as to whether he should be considered a covid fatality and the medical consensus was he shouldn't because he was dying this week regardless of whether he caught it or not, and also, the official cause of death was one of his other major issues, but tin foil hat wearers are crying conspiracy (much like some on here with the German figures based on news stories and no further understanding).
As this affects the old and sweeps through hospitals there are going to be some people specifically killed by C19 but there are presumably going to be a not insignificant number of people who catch it and then die of whatever they were in there for in the first place, possibly at little earlier than otherwise expected but sometimes, presumably not.
It must be reasonably straight forward to account of the number of deaths that would be expected to occur without covid, for example, there must be a rough figure for how many elderly people are expected to die from flu, if the current number is half that I think it is a little disingenous to discount that in terms of the effect C19 is having on society.
The problem is with everyone on lock down there is no other news so the media are focusing on this and for some reason feel vindicated if they sensationalise something and then finish with a piece of people clapping nurses
The COVID-19 official count also does not include people who die from other diseases because hospitals are overloaded and can't get adequate care as a result. When a heart attack patient who would have lived under normal conditions has to wait 2 hours and dies, that doesn't count in the COVID-19 stats.
Same principle in reverse can be used to account for these**
** I'm not suggesting it should be done in real time as there are obviously more important things to worry about
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 7:23 am
by goeagles
Clogs wrote:
I think where you are getting to is that the first case in Italy was way way before the 31st of Jan. Even way before the 15th of Jan.
Some high tech Photoshop work to visually demonstrate...
No, what I’m getting at is that their methodology is garbage. Ignoring fat tailed distributions due to superspreaders will completely screw up your growth as the amount of superspreaders early on greatly impacts how fast things grow. It’s even possible that the first seed never causes an outbreak and requires later seeds due to low R0.
But want the easiest example that their 0.01% number, and transitively their methodology, is nonsense? More than 0.01% of the entire population of Italy has already died.
Re: Coronavirus Thread. Virus v humans
Posted: Fri Mar 27, 2020 7:30 am
by goeagles
MrJonno wrote:goeagles wrote:MrJonno wrote:With regards to the numbers I think a lot of people are taking a rather simplistic approach. Recently a man in his 90s in the Czech Republic who had numerous underlying health issues, was clining on to life and expected to expire any minute, caught covid 19 and then 'moved on'. There was some debate as to whether he should be considered a covid fatality and the medical consensus was he shouldn't because he was dying this week regardless of whether he caught it or not, and also, the official cause of death was one of his other major issues, but tin foil hat wearers are crying conspiracy (much like some on here with the German figures based on news stories and no further understanding).
As this affects the old and sweeps through hospitals there are going to be some people specifically killed by C19 but there are presumably going to be a not insignificant number of people who catch it and then die of whatever they were in there for in the first place, possibly at little earlier than otherwise expected but sometimes, presumably not.
It must be reasonably straight forward to account of the number of deaths that would be expected to occur without covid, for example, there must be a rough figure for how many elderly people are expected to die from flu, if the current number is half that I think it is a little disingenous to discount that in terms of the effect C19 is having on society.
The problem is with everyone on lock down there is no other news so the media are focusing on this and for some reason feel vindicated if they sensationalise something and then finish with a piece of people clapping nurses
The COVID-19 official count also does not include people who die from other diseases because hospitals are overloaded and can't get adequate care as a result. When a heart attack patient who would have lived under normal conditions has to wait 2 hours and dies, that doesn't count in the COVID-19 stats.
Same principle in reverse can be used to account for these**
** I'm not suggesting it should be done in real time as there are obviously more important things to worry about
Look at the total deaths for a week for a region with an outbreak and compare to that same week’s average over the last 5 years. Small sample size, but something like this:
